FCTC: successes and gaps
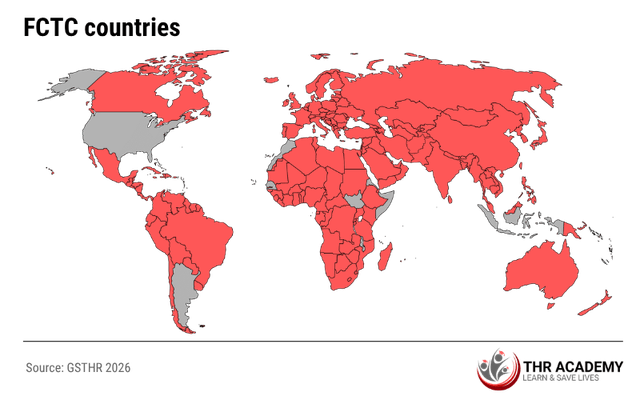
The Framework Convention on Tobacco Control (FCTC) is the world’s first global public health treaty, adopted in 2003 under the auspices of the World Health Organization and entering into force in 2005. It provides countries with a shared legal and policy framework for reducing both the demand for and supply of tobacco through evidence-based measures. As of 2024, 183 countries are Parties to the FCTC, covering more than 90% of the global population. This makes it one of the most widely adopted international health treaties to date.
What has the FCTC achieved?
Over the past two decades, the FCTC has delivered several important gains:
- It has established a global standard for tobacco control, covering taxation, advertising bans, packaging, and smoke-free environments.
- It has strengthened political commitment, prompting many countries to create national tobacco control programmes and coordinating bodies.
- It has driven legislative action, including large graphic health warnings, smoke-free public spaces, and restrictions on advertising, promotion, and sponsorship.
- It has improved accountability, supported by regular reporting and monitoring through tools such as the MPOWER framework.
- In countries that implemented its provisions comprehensively, especially middle- and high-income countries, it has contributed to meaningful reductions in smoking prevalence.
Where does the FCTC fall short?
Despite these successes, the impact of the FCTC has been uneven, particularly in low- and middle-income countries (LMICs). Several challenges continue to limit its effectiveness [^1]:
- Many LMICs lack the funding, technical expertise, and enforcement systems needed for full implementation.
- Article 14, which calls for accessible help to quit tobacco use, remains the least implemented provision globally. It has been reported that fewer than one-third of high-income countries offer comprehensive cessation support, and fewer than one in ten middle-income countries provide such services [^2].
- Protections under Article 5.3 are often poorly enforced, allowing industry influence over policy in many settings.
- Incomplete or outdated data systems reduce accountability and slow progress.
- While some upper-middle-income countries have implemented the treaty robustly, low-income countries often lag due to competing health priorities and donor dependence.
- Harm reduction is mentioned in the FCTC but has never been developed as a core element of tobacco control, resulting in ongoing policy ambiguity around lower-risk nicotine products.
The FCTC remains a landmark achievement in global health, but ratification alone is not enough. Its future success depends on sustained political commitment, adequate funding, and approaches that reflect the realities of LMIC contexts.
As this course will explore, integrating harm reduction alongside traditional tobacco control measures may offer a more realistic and equitable pathway to reducing tobacco-related harm, particularly where progress has stalled [^3].
-
Chung-Hall J, Craig L, Gravely S, Sansone N, Fong GT. Impact of the WHO FCTC over the first decade: a global evidence review prepared for the Impact Assessment Expert Group. Tob Control. 2019 Jun;28(Suppl 2):s119-s128.
-
Batini C, Ahmed T, Ameer S, Kilonzo G, Ozoh OB, van Zyl-Smit RN. Smoking cessation on the African continent: Challenges and opportunities. Afr J Thorac Crit Care Med. 2019 Jul 31;25(2):10.7196/AJTCCM.2019.v25i2.015.
-
Adebisi YA, Jimoh ND, Ogunkola IO, Olayemi A, Omolayo AT, Oyedokun D. Tobacco control needs a choice-based approach to curb cigarette smoking. Ann Med Surg (Lond). 2022 Jul 13;80:104186.